
T1D is highly heritable and tends to manifest at an early age. One application of this predictor is to differentiate between T1D and the more common (in later life) T2D. Another application is to embryo screening. Genomic Prediction has independently validated this predictor on sibling data and may implement it in their embryo biopsy pipeline, which includes tests for aneuploidy, single gene mutations, and polygenic risk.
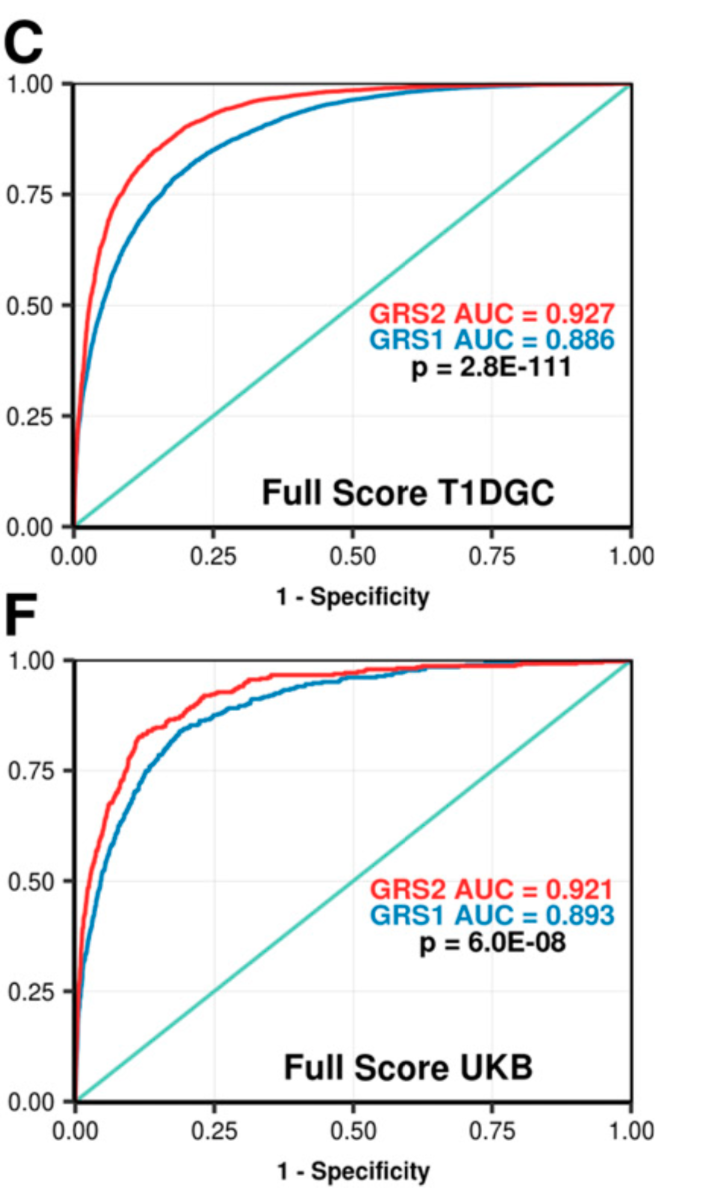
Development and Standardization of an Improved Type 1 Diabetes Genetic Risk Score for Use in Newborn Screening and Incident DiagnosisThe figure below gives some idea as to the ability of the new predictor GRS2 (panels B and D) to differentiate cases vs controls, and T1D vs T2D.
Sharp, et al.
Diabetes Care 2019;42:200–207 | https://doi.org/10.2337/dc18-1785
OBJECTIVE
Previously generated genetic risk scores (GRSs) for type 1 diabetes (T1D) have not captured all known information at non-HLA loci or, particularly, at HLA risk loci. We aimed to more completely incorporate HLA alleles, their interactions, and recently discovered non-HLA loci into an improved T1D GRS (termed the “T1D GRS2”) to better discriminate diabetes subtypes and to predict T1D in newborn screening studies.
RESEARCH DESIGN AND METHODS
In 6,481 case and 9,247 control subjects from the Type 1 Diabetes Genetics Consortium, we analyzed variants associated with T1D both in the HLA region and across the genome. We modeled interactions between variants marking strongly associated HLA haplotypes and generated odds ratios to create the improved GRS, the T1D GRS2. We validated our findings in UK Biobank. We assessed the impact of the T1D GRS2 in newborn screening and diabetes classification and sought to provide a framework for comparison with previous scores.
RESULTS
The T1D GRS2 used 67 single nucleotide polymorphisms (SNPs) and accounted for interactions between 18 HLA DR-DQ haplotype combinations. The T1D GRS2 was highly discriminative for all T1D (area under the curve [AUC] 0.92; P < 0.0001 vs. older scores) and even more discriminative for early-onset T1D (AUC 0.96). In simulated newborn screening, the T1D GRS2 was nearly twice as efficient as HLA genotyping alone and 50% better than current genetic scores in general population T1D prediction.
CONCLUSIONS
An improved T1D GRS, the T1D GRS2, is highly useful for classifying adult incident diabetes type and improving newborn screening. Given the cost-effectiveness of SNP genotyping, this approach has great clinical and research potential in T1D.

No comments:
Post a Comment